
Frenectomies and Ankyloglossia
All of the following terms are correct spelling and can be found in many medical dictionaries:
- Frenulum (s)
- Frenum (s)
- Frena
- Frenotomy
- Frenectomy
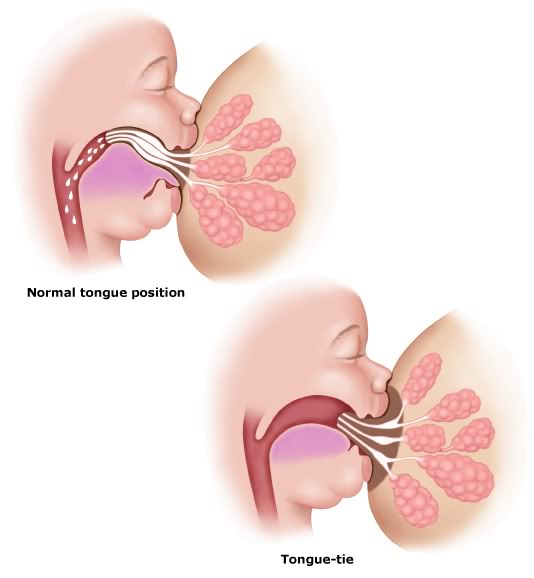
- Tongue-tie
- Tongue tied
A frenum is a band of muscle or fascia that attaches the lips, cheeks, or tongue to underlying bone of the upper or lower jaw. They appear to play a minimal role in the function of the tongue or muscles of facial expression and the lips as when they are removed, there is no significant reduction of these muscles.
Frenum and Tongue Tie Problems
Less than 1% of upper lip or tongue frenums cause problems and require surgical removal either during childhood or as an adult. However, when a frenum ligament is too short, attached too high on the jaw bone, or wraps around the jaw bone as seen in the upper jaw, the following issues can develop in babies, children and adults:
- Inability of neonates to suckle (breastfeed)
- Localised gum recession of the upper or lower incisors. Occasionally a tongue frenum can strip the gum on the lower front teeth causing considerable pain and discomfort.
- Midline gap between the two upper maxillary central incisors
- Speech and chewing difficulties:
- Difficulties can include creating sounds that need the tongue or tongue tip to touch the roof of the mouth, to pronounce sounds such as ‘t, d, n, l, s, z’
- arch off the floor of the mouth, to pronounce sounds such as ‘r’
- Unable to protrude or move the tongue from side to side
- Can cause problems with food regularly getting caught under or down the sides of the tongue, and cannot be cleared from the sides of the mouth
- Facial growth deficiencies
- Orthodontic malocclusions and dental crowding
- Interference with denture fabrication / wear in older adults
- Mouth breathing habits
- Snoring / sleep apnoea
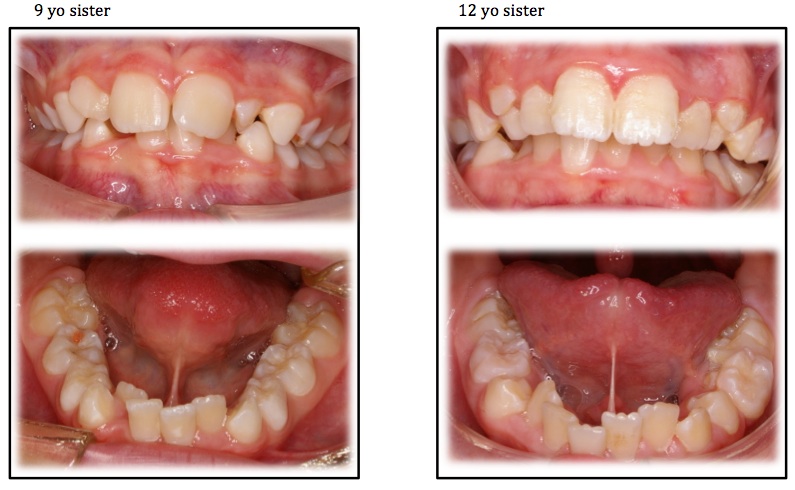
Images show almost identical dental malocclusions (crowding) on two sisters aged 9 and 12 as a result of untreated tongue tie
Fenectomy Fact Sheet
![]() Please use this fact sheet for further information and treatment of frenectomies
Please use this fact sheet for further information and treatment of frenectomies
Breast Feeding
When a baby has a tongue tie or tight upper lip frenum it often is unable to suckle or breastfeed properly due to not being able to form an adequate or inefficient lip seal on the nipple of the mother. This can cause nipple trauma and pain when the nipple is compressed against the gums of the baby rather than the tongue. It is also a major contributor to mastitis (a painful inflammation of the breast / nipple). The baby’s tongue that is ‘tied’ is unable to perform a ‘wave’ motion that is required to obtain milk from the mothers breast. A tongue and lip tie therefore can cause the baby to have lengthy and excessive feeding times, require ‘finger feeding’ using very small amounts of frozen breast milk repetitively throughout the day and night, develop regular aerophagia (wind), experience regular stomach upset and reflux, have a failure to thrive and gain weight, and contribute to the later development of mouth breathing habits.
 Signs that a baby could be tongue-tied include that:
Signs that a baby could be tongue-tied include that:
- the mother has sore nipples during and after breastfeeding
- when elevated, the upper lip ‘blanches’ (turns white) around the frenum, gums, or lip
- the mother has squashed nipples after breastfeeding
- the mother has a white compression mark on the nipple after breastfeeding (from excessive pressure of the baby trying to form a mouth seal on the breast)
- the baby has difficulty latching on to the nipple with or without the use of nipple shields
- the baby detaches from the nipple regularly during feeds
- the baby often loses suction while feeding and sucks air (aerophagia)
- the baby’s mouth makes a clicking sound while feeding
- the baby tires very quickly during feeding
- the baby fails to or is slow to gain weight
- regular reflux or vomiting during and after feeding.
As a result of tongue and lip ties, the baby is often switched to a bottle in an attempt to feed adequately without debilitating pain and discomfort that is caused to the mothers breast. Also, many mothers find they travel from practitioner to practitioner including paediatricians, GP’s, dentists, lactation consultants and speech pathologists and the tongue and or lip ties is not identified as being the major contributor to the feeding problem, or it is dismissed as being an ‘important’ cause. As we work very closely with speech pathologist Ms Holly Puckering and various lactation consultants, we see babies from all over Tasmania often on referral from other health practitioners, and so parents can be assured their baby is in safe and very experienced hands.
ABC Radio Interview on Tongue Ties with Hobart Speech Pathologist Ms Holly PuckeringTongue Ties
Speech
Many children can develop a speech problem due to tongue ties that are not removed in the early years of development. Depending on the severity of the tongue tie dictates the impact on speech. Often, on removal of the tongue tie a short period of speech pathology is required and most speech problems are resolved.
Tongue Tie Surgery
The removal of a tongue-tie is a relatively simple procedure and varies in tehcnique depending on the age of the infant, child, or adult. It must be performed by an experienced clinician whom has a solid understanding of the anatomy of the mouth and tongue given the proximity of the saliva ducts, nerves, and arteries in the floor of the mouth. If not performed properly by a practitioner with considerable experience in frenectomies, excessive trauma and pain to the person or baby can result, or vital anatomical structures such as saliva ducts and nerves to the tongue can be damaged for life.

Dental Soft Tissue Laser
With infants it simply involves releasing the tongue tie with a small pair of sterile scissors or a soft tissue laser. There is very little if any bleeding, and the release site typically heals very quickly without any complications. Often the baby will not even know the procedure has been performed, whilst others may cry for a minute or two until being comforted and settling quickly. The improvement to tongue range of motion is almost immediate with many babies being able to breastfeed soon after the procedure.
Most babies seen for tongue tie procedures at our practice are typically seen immediately afterward and in conjunction with a speech pathologist and lactation consultant who provide post operative care and breast feeding techniques in the complete privacy of a dedicated room. This is to ensure that the baby is feeding correctly before both mother and baby head home.
In children and adults, the procedure is typically conducted under local anaesthetic. Again it is a very quick and painless procedure. The frenum is removed surgically, and several stitches may be placed if required. When a soft tissue laser is used, stitches are not require as the area bleeds very little. The frenectomy site typically heals very quickly and is no more uncomfortable than having a mouth ulcer, or having bitten the inside of a cheek for several days. Very rarely complications such as infection may occur which are promptly treated as required.

Upper Lip Frenum
Frenums in the upper lip can be classified as I – IV.
Class I frenums attach to the gum above the teeth and is the normal position for the majority of people. These cause no problems with position or function of the upper incisors and upper lip.
Class II frenums attach to the gum just above the upper central incisors. These can cause a space to develop between the teeth (diastema), but typically as the person ages into their teens, the frenum recedes upwards and no treatment is required. The diastema often closes spontaneously as adult teeth continue to erupt.
Class III frenums attach in-between the upper central incisors and can cause mild to moderate diastemas. Variations in the severity of diastema can occur due to the thickness of band of tissue from the frenum that may differ from person to person. The frenums require surgical removal, and often orthodontic treatment may be required to close the diastema. Typically however, once the frenum is removed the diastema will spontaneously close over time.
Class IV frenums attach to the anterior papilla or behind the upper central incisors. The frenums cause considerable diastema’s to occur due to the thickness of the band of tissue present between the teeth acting like a rubber band. Surgical removal of a Class IV frenum is required if any orthodontics is considered to close the diastema. If the frenum is not removed, as soon as the orthondontic braces are removed the upper central incisors will spring apart again very quickly.

Class 1 Frenum

Class 2 Frenum

Class 3 Frenum

Class 4 Frenum