
Like any joint in the body, the TMJ’s are subjected to wear and tear, trauma (micro and macro), disease, degeneration, and growth and developmental abnormalities over time.
Arthritis
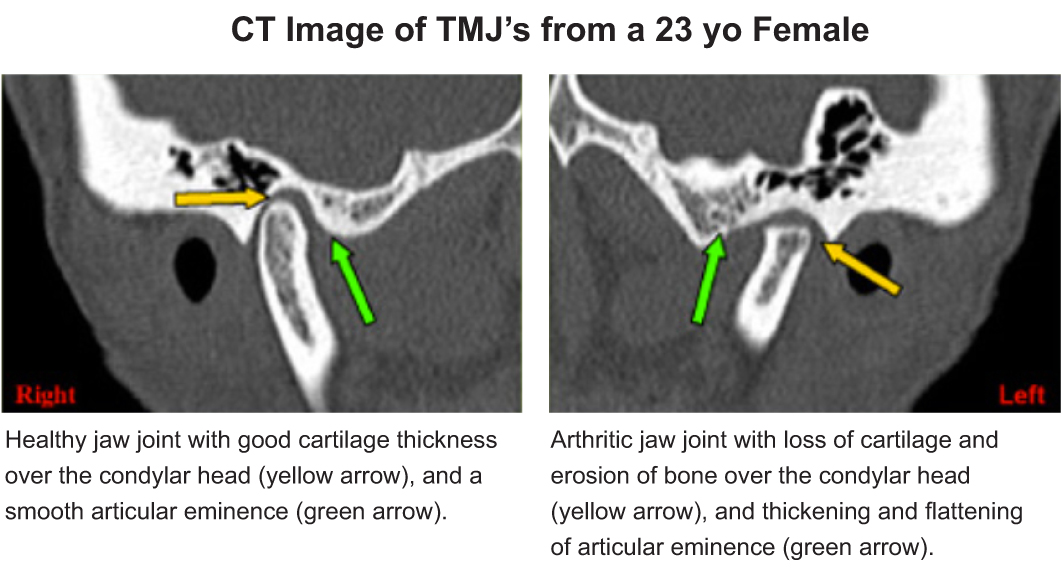
Arthritic changes occur when there is a breakdown of the articular surfaces of the joint that leads to degeneration and an inflammatory condition that can affect any joint in the body. Various forms of arthritis such as Osteoarthritis (degenerative), Rheumatoid, Infectious, Psoriatic and others can all cause pain in the TMJ’s. Repetitive micro and macro trauma can also cause degeneration of the TMJ’s. The prevalence of arthritic changes in the jaw joints increases with age but by no means is restricted to an elderly population. Primary arthritic disease is seen in older people from wear and tear and is usually asymptomatic. When symptoms do occur they often present as mild complaints with some developing into severe pain and limited mouth opening.
Secondary degenerative arthritis occurs as a result of trauma or chronic clenching and bruxing and is usually seen in younger people. The presenting symptoms are often much more severe than seen in primary arthritis.
Bruxism
Generally, bruxism (grinding of the teeth) occurs when a person is asleep which is why so many people do not even realise they do it. Forces generated during sleep bruxism can be extremely high and cause significant damage to the teeth and trauma to the supporting bone and tissues. This damage can be obvious, whilst in many other people it is a low grade but chronic and repetitive condition. Injury to the TMJ’s can develop from this constant grinding of the teeth from excessive forces to the ligaments, disc, and articulating surfaces of the jaw joints. At the very least, bruxing will typically produce muscle pain in the face and sore jaw muscles, especially when waking in the morning.
Clenching In many ways clenching of the teeth can lead to much more painful conditions than bruxing and is even more difficult to diagnose.
Teeth should never contact except lightly during chewing.
When teeth are held together or the jaw is held tense over a period of time such as when concentrating, or during periods of stress or anxiety, the facial and neck muscles become fatigued and painful.
Morning and afternoon headaches, difficulty chewing, neck pain, and sore facial muscles are the most commonly reported symptoms. When clenching becomes chronic such as day and night, many severe muscle-related symptoms can occur that can have dramatic effects on a patient’s quality of life. This leads to a painful muscle condition called myofascial pain syndrome and is the MOST common cause of facial, neck, and shoulder pain in persons suffering from a TMJ disorder.
Growth and Development
The TMJ’s are a part of the body and as such are also subject to problems such as tumours, abnormal growth, developmental delays, syndromes, and diseases. Although relatively rare, congenital and developmental anomalies, and neoplasms of the TMJ are important to identify early in life to re-establish normal growth of the mid-face, and in adults to limit the amount of change and destruction that can occur within the facial bones and TMJ’s. Other diseases can also affect the TMJ’s and cause facial and jaw pain.
Conditions and diseases that can occur include:
Condylar agenesis
Condylar hypoplasia
Condylar hyperplasia
Hemifacial microsomia
Ankylosis of the TMJ
Sjogren’s Syndrome
Systemic Lupus Erythematosis
Scleroderma
The most common tumours of the TMJ’s are benign and include:
Chondromas
Osteomas
Osteochondromas
Rarely seen are Fibrous Dysplasia, Giant Cell Reparative Granuloma, and Chondroblastoma. Even less frequently seen are the malignant Fibrosarcoma and Chondrosarcoma.
Muscle overactivity
When the muscles of the head and neck are overused, just like any other muscle in the body, pain will develop. The muscles that most commonly become tender that will cause facial and TMJ pain and headaches are the Masseter, Anterior Temporalis, Medial Pterygoid, Trapezius, and Sternocleidomastoid muscles.
Muscles of the head, neck, and jaw represent a very large part of TMJ disorders and presenting pain symptoms
Overuse of the facial and neck muscles can develop from teeth clenching and grinding, habits that cause the jaw to be held in an abnormal position or for long periods such as pen/pencil chewing, violin playing, lip and nail biting, resting your chin in the palm of your hand, and poor body posture such as a forward head position.
Recognised disorders of the head and neck muscles are characterised by pain from pathological or functional changes in a muscle group. They include:
Myositis – an acute condition with inflammation of the muscle and its connective tissue attachments that results in pain, swelling, and a decreased range of motion. Causes include overuse, infection, or trauma.
Muscle spasm – is an acute contraction of a muscle caused by overuse or overstretching of a muscle. It is often referred to as ‘guarding’ following an acute injury. If left untreated, muscle spasm in the contracted state can result in fibrous scarring and permanent contracture of the muscle will develop.
Trismus – is a decreased range of motion due to infection or psychological causes (hysterical trismus). Trismus can also occur after dental injections.
Fibromyalgia – diffuse, firm, painful muscular bands (trigger points) develop and are often associated with a sleep disorder and general chronic pain states. Pain follows known referral patterns of these trigger points and can often be reproduced by applying pressure to them.
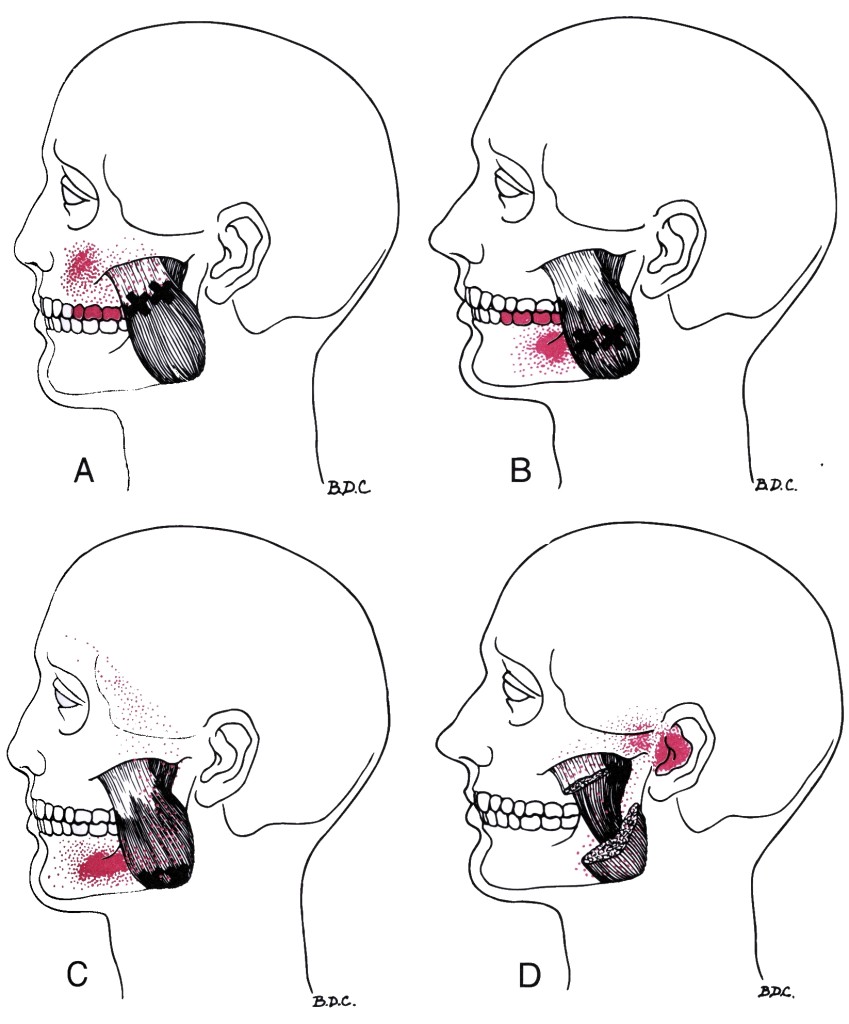
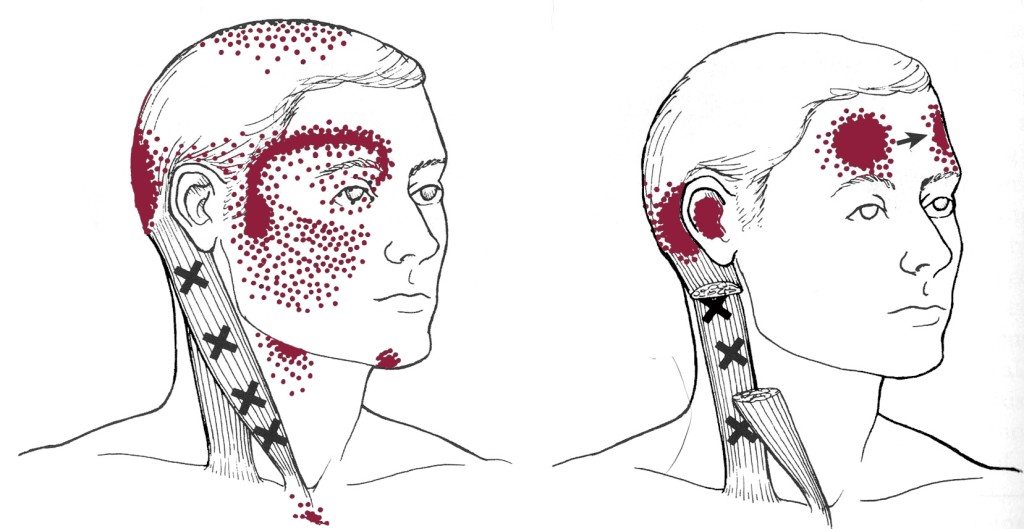
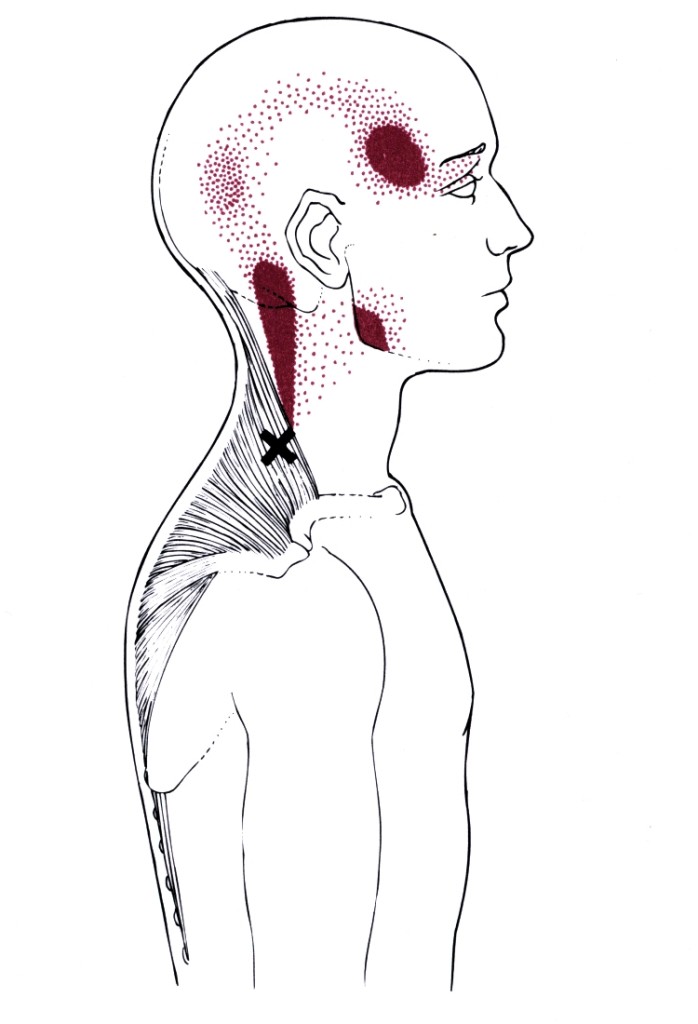
Examples of Trigger Points:
In all of the following examples, the black X marks where in the muscle the central trigger point can be found, whilst the solid red shaded area is the main pattern of referred pain. The stippling or ‘dotted’ red areas are the spill over of referred pain. (Images reproduced from Travell and Simons).

Synovitis
A synovial membrane lines the TMJ and produces a fluid that lubricates the joint and allows it to function smoothly. An inflammatory condition of the synovial membrane will produce pain and can cause limited movement within the TMJ. Rheumatoid arthritis can cause a synovitis in the TMJ’s.
Trauma
Macro trauma such as motor vehicle accidents, assaults, sporting injuries, falls, difficult dental and wisdom tooth extractions, and any other incident where a sudden blow, shock, or hyperextension injury to the jaw joints occurs, can cause a TMD. In the majority of cases, macro trauma will cause an immediate level of pain and concern that requires urgent treatment such as a blow to the side of the head, or a fall. In some cases however, the initial precipitating injury often may be very subtle and occur years previously, and even as a child. The injury can therefore be overlooked as symptoms resolve over a period of weeks, but may return or develop later in life to a level that treatment is sought.
Micro trauma is a consistent and repetitive low-level grade of stress to the TMJ system over a period of time. It most commonly occurs as a result of continual teeth clenching and teeth grinding that overwhelms the TMJ’s shock absorber ability to tolerate the forces that are generated. A majority of microtrauma occurs when we sleep, as this is when forces from teeth clenching and grinding are at their greatest. However, a considerable amount of microtrauma can occur during the day, and it is this factor that remains incredibly overlooked and undertreated in the dental and medical professions.
Occlusion
Contrary to many popular advertised and purported myths on dental websites, occlusion or a patients bite is NOT a cause of TMD.
Unfortunately for many patients they are informed that they require expensive dental treatment such as implants, crowns / bridges, occlusal rehabilitation, and orthodonticts to ‘fix’ their TMD complaint, or they undergo repetitive ‘occlusal adjustments’. This advice and forms of treatment are often far from the truth and very misleading. These people then spend large sums of money having the treatment conducted, only to be left with the original TMD pain complaint when the ‘cause’ of their pain and symptoms has been left undiagnosed or untreated. Or worse, their underlying condition was completely misdiagnosed.
Missing teeth, severely worn teeth, poorly fitting dentures, and malocclusions can however all be ‘associated’ with developing a TMD, whilst not being a direct cause. For many people that develop a TMD they also have these problems with their bite, and may require treatment to stabilise the TMJ’s long term when there are ‘intra-articular’ joint problems such as arthritis, clicking, grating / grinding noises (crepitus). Any proposed dental treatment should occur ONLY in conjunction with a comprehensive TMD pain management and rehabilitation plan after a correct diagnosis of the pain ’cause’ has been made.
“80 – 90% of TMD pain is muscular and does not involve an intra-articular TMJ problem.”
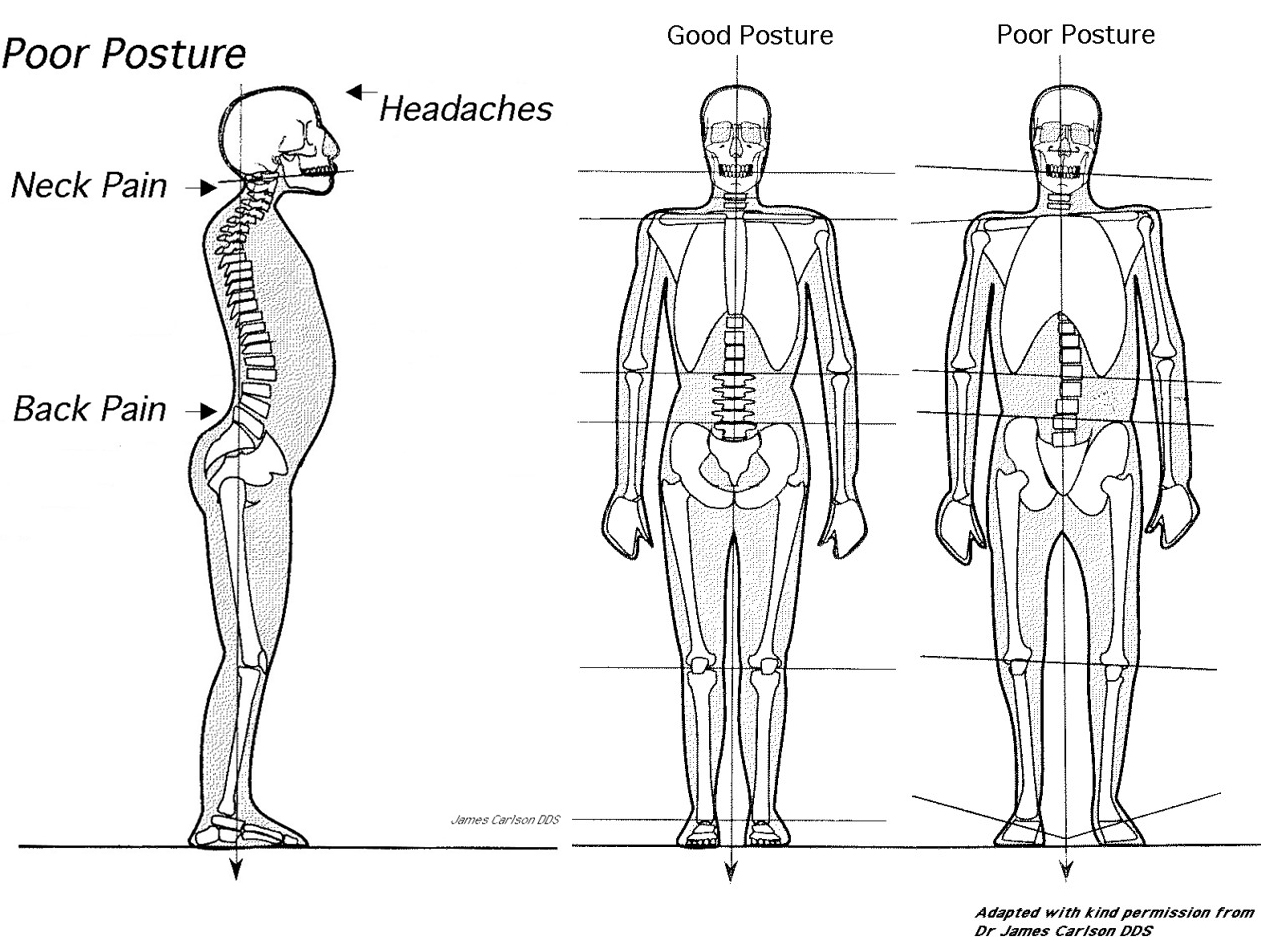
Body Posture and TMD
Many studies over the past decade have shown that a relationship exists between your teeth and bite, your jaw joints, head position, head and neck muscles, lower back, pelvis, your feet, and your general upright standing posture. The musculoskeletal system therefore can often be a factor in many types of pain or functional conditions, and a problem in any one of these areas may, and often does contribute to a problem in another part of the body.
Poor posture, particularly of the head and shoulders results in overactivity of the muscles that support these parts of the body and leads to fatigue, pain, and trigger points. A forward head posture is a major contributor to headaches that occur in the afternoon. Assessment, treatment, and long-term management of TMD symptoms requires focus on and correction of postural problems to help adequately reduce muscle-orientated pain and dysfunction.
 Snoring and Sleep Apnoea
Snoring and Sleep Apnoea
Increasingly, research is showing that the airway and sleep disorders are major factors that contribute to patients developing a TMD and chronic orofacial pain problems. In those people who snore or have Obstructive Sleep Apnoea (OSA), excessive tooth grinding may occur as the jaw is constantly pushed forward during sleep in an attempt to open the airway and this condition is known as Sleep Bruxism. Over time, excessive tooth loss and constant forces on the facial muscles and TMJ’s can lead to pain and dysfunction.
In our practice, a retrospective study showed that approximately 30% of patients with TMD had an undiagnosed sleep disorder of some kind. And the same applies to patients who suffer from snoring and sleep apnoea. Approximately 10% have a jaw joint problem or have excessive tooth wear that needs to be addressed and managed whilst treating the sleep disorder. For many people, chronic sleep deprivation from bruxism, clenching, snoring, OSA, and general chronic pain causes a continued never-ending cycle of excessive daytime sleepiness, increases in stress and anxiety, and an increase in pain. Without addressing the sleep dysfunction, it is often impossible to fully resolve pain complaints.
Orthodontics
There is still much debate and controversy that continues to rage around the world regarding orthodontics and the development of TMD problems, especially with regards to “extraction approach orthodontics” where four adult premolars are often removed to create straight teeth. This form of orthodontics often retrudes (pulls backward) the upper teeth and forces the lower jaw into a backward position when the teeth are closed together. As a result, the jaw joint itself and the muscles of mastication are forced into an unfavourable and very uncomfortable long-term position and relationship. It has also been suggested in scientific literature that extraction orthodontics may contribute to the development of snoring and OSA in adults as the lower jaw is pushed backwards and proceeds to constrict the airway.
This remains controversial, but is certainly being regarded as plausible, and even accepted more recently as fact when the hard and soft tissue anatomical changes of the face, jaws, and throat that can occur during extraction orthodontics is reviewed in depth.
Many orthodontists will swear that orthodontics and removing adult teeth has nothing to do with the development of a TMD and in no way causes any problems. Apart from the unfavourable facial profiles that usually occur in persons with extraction orthodontics, comments to patients that present with a TMD during the course of or soon after completion of extraction orthodontics such as “You will grow out of it”, “It is only muscle spasm”, “You are just a bit stressed”, and other similar unrelated explanations of the persons TMD symptoms can be very misleading and do nothing to assist the person’s presenting symptoms.
Fortunately there are not too many orthodontists who continue to hold this view as the general current consensus is that there are certain people who may be ‘at risk’ of developing a TMD during orthodontic treatment, just as there are people at risk of developing many other types of health problems. This view is likely to be a more accurate evaluation of the relationship between extraction orthodontics and TMD.
It is very unfortunate that extraction orthodontic approaches continue to be a widespread practice for many children. When a TMD is identified before, during, or soon after orthodontic treatment however, it is very important that the patient tells the treating orthodontist so that the TMD can be assessed and treated immediately.
It is through Dr Eldridge’s extensive clinical experience that he has formed the personal view that extraction orthodontic approaches should be avoided wherever possible* as this may place at risk ‘susceptible’ patients from developing a TMD. It may also lead to a snoring or OSA condition later in life or significantly worsen an already existing sleep disordered breathing problem. These opinions are inline with an increasing number of research findings and best practice medicine. Treatment of people with a history of extraction orthodontics often then involves attempting to re-establish the patient’s jaw and tooth position to where they would have been before the extractions.
For cases where orthodontics is required either before or after TMJ treatment to stabilise a jaw position, or provide a more favourable occlusion, here at the Orofacial Pain and Special Needs Clinic, Dr Eldridge prefers to use the Invisalign system of orthodontic treatment. This enables Dr Eldridge to keep tight control over the entire phases of treatment and final position of the teeth and jaw joints.
*Not all orthodontic cases can avoid extractions of adult teeth when they are associated with severe levels of crowding. In general however, extractions create far more space than is required to fix the crowding. Space / crowding discrepancies should always be discussed with the treating orthodontist before treatment commences and if any questions persist regarding the need for extractions, a second opinion from a non-extraction orthodontist should be sought.