
Treatments
If an internet search is performed using the string ‘snoring’ or ‘obstructive sleep apnoea / apnea (OSA)’ you will be swamped with treatment options for these two conditions that range from pillows, nasal sprays, breathing exercises, weight-loss pills, over the counter nose strips, and meditation CD’s, to the more scientifically and researched evidence-based treatments such as Continuous Positive Airway Pressure (CPAP), mandibular advancement appliances, and surgery.
The treatment of snoring and Obstructive Sleep Apnoea (OSA) is not performed in a ‘One Stop Shop’ or by purchasing a product from the Internet. It is often a condition that occurs from a multifactorial cause i.e. from a combination of weight gain, genetics, throat tissue architecture, nasal obstructions, diet, allergies, medical conditions, and so forth. Therefore, in many cases, only addressing one of the causes is not enough to treat the snoring or OSA. Often, a combination of treatments is required to achieve maximum medical improvement of a person suffering from a sleep disorder.
“There ain’t no way to find out why a snorer can’t hear himself snore.”
– Mark Twain
Oral Sleep Appliances
The use of oral appliances to hold the mandible (lower jaw) forward during sleep for the treatment of snoring and mild to moderate OSA is a scientifically proven and effective method. The American Academy of Sleep Medicine (AASM) recently reviewed its 1995 practice parameter guidelines on the use of Oral Appliance Therapy (OAT) recommending it as a first line of treatment in specific circumstances of Snoring and OSA. These updated guidelines by Kushida et. al. appeared in the February 2006 issue of the journal Sleep.
Although they may not always be as efficacious as CPAP for severe OSA, according to these guidelines, for patients with snoring or mild to moderate OSA, those who cannot tolerate CPAP, fail treatment attempts with CPAP, are unwilling to use it, or do not respond to CPAP, and those who fail treatment attempts at weight loss and changes in sleeping position, oral appliances may certainly be indicated in all of these people.
In more severe cases of OSA when CPAP cannot be tolerated or very high pressures are required, OAT may be used as a replacement for or in conjunction with CPAP. The decision to cease using CPAP however, and the benefits of its use compared with the adverse health effects of severe sleep apnoea should always be considered very carefully.
How Do Oral Appliances Work?
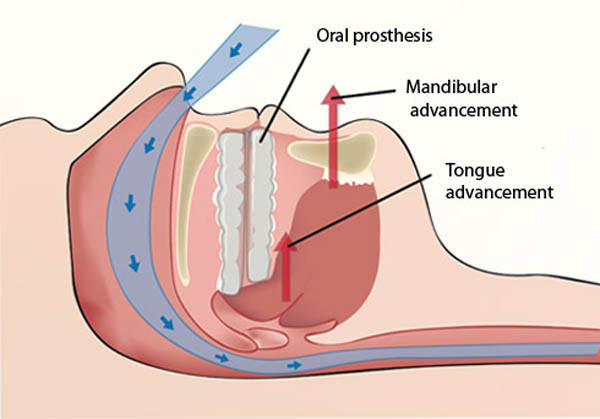
Oral appliances (or Mandibular Advancement Splints) are worn on the upper and lower teeth during sleep and hold the lower jaw forward thereby helping to prevent the tongue and the soft tissues of the mouth and throat from collapsing.
By wearing the appliance during sleep, adequate air intake occurs and helps provide normal regular sleep that is free from snoring, obstructions, and respiratory related arousals. Appliances can be used by themselves or in conjunction with other treatments such as surgery or Continuous Positive Airway Pressure (CPAP) systems. Designed properly for each individual patient and their specific circumstance, oral appliances are safe, effective, comfortable, and have very few side effects.
There are basically two types of oral appliances on the market.
1. Non-adjustable: These are essentially two mouthguards joined together that fit over the upper and lower teeth and hold the jaw forward in one position only. Many variations of one-piece oral appliances are available on the market and these are most often sold over the Internet or constructed by denture technicians and denture prosthetists.
Boil & Bite non-adjustable.
“Boil and Bite” appliances, and one-piece appliances are cheap and often the optimal position of the lower jaw is a pure guess for patients and dentists. It is these types of appliances that most of the problems with jaw joints, muscle pain, and poor efficacy result from, as fitting and function is not professionally and expertly carried out. Many people may then give up on OAT without seeking a proper assessment and appliance.
2. Adjustable: Current research has proven that adjustable appliances are far more superior, effective, and comfortable in the treatment of snoring and OSA. The most comfortable appliances are constructed by taking impressions of the patient’s teeth and positioning the jaw forward slowly in increments until the ideal position is achieved. Often movements of only 1mm are required to bring the patient from “I am still snoring with this appliance” to “I feel great in the morning and my partner is very happy”.
Somnomed MAS fully-adjustable. Appliances can also be constructed for patients with no upper teeth.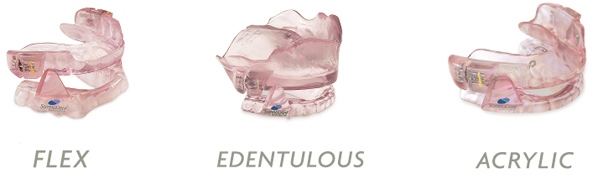
Adjustable appliances also have the added benefit of protecting the teeth from bruxing and being customisable to include additional components and design for retention, tongue positioning, lip seal, and jaw joint problems. These appliances can also be used in the simultaneous treatment of severe TMD cases when the practitioner has considerable experience in this area. Dr Eldridge has successfully treated many hundreds of people with severe TMJ disorders and OSA when other specialists have told them that an oral appliance is contraindicated.

3. Tongue Retaining Devices: These appliances are designed to allow the tongue to remain in a forward position between the anterior teeth by holding the tongue in an anterior bulb with negative pressure, during sleep. This pulls the tongue forward to enlarge the volume of the upper airway and to reduce upper airway resistance. Tongue retaining devices are used mainly for people with no natural teeth. Results vary greatly between different people due to comfort factors.
Treatment with Oral Appliances
Oral appliance therapy for the treatment of Snoring and OSA is a very reliable and efficacious mode of therapy when carried out professionally and with expert knowledge. Initial consultations and assessments when performed properly and thoroughly take around 1 hour on average. Successful snoring and OSA treatment is typically not isolated to just mandibular advancement devices, or a ‘magic plastic cure’ using a one size fits all approach such as ‘off the shelf boil and bite’ appliances.
Sleep disorders must always be considered and assessed intimately with lifestyle issues such as diet, weight – loss and exercise, soft-tissue architecture, the temporomandibular joints, oral health, the occlusion, and general health including any existing medical conditions and medications. A working relationship therefore between Respiratory Physicians, Ear Nose and Throat surgeons, General Medical Practitioners, and a Dentist who has specific knowledge, training, and experience in treating sleep disorders is essential to successful team management of patients with snoring and OSA and returning the person a much improved quality of life.
When designed and used correctly, oral appliances function by advancing the mandible and pulling the tongue off the back of the throat. Simultaneously, by advancing the mandible the muscles of the back of the throat open by tightening width ways. The result is that the tongue, soft palate, and the walls of the throat tighten and open to allow more air to enter through the nose and mouth by reducing or removing the blockage that was causing snoring and sleep apnoea.
Patients treated with oral appliances should return at strict regular scheduled intervals to monitor patient adherence, allow adjustment of and evaluate deterioration of the appliance, and to evaluate the oral tissues, joint structures, and occlusion. Regular follow up is also needed to assess the patient for signs and symptoms of worsening OSA.
Sleep breathing disorders can contribute to severe life threatening medical complications and so it is our priority to provide you with a ‘Long-term Treatment Plan’, and not just a treatment.
CPAP
Positive airway pressure systems maintain the upper airway patency during sleep by forming a pneumatic ‘splint’. This pressure prevents the airway from collapsing by pumping air via a mask attached to the machine by a hose.

The constant air pressure, usually around 5-20 cmH20 (centimeters of water) is delivered throughout the breathing cycle. Most patients do well with 8-10 cmH20 air pressure. The exact pressure required for each individual patient is normally assessed in the first instance during an overnight Polysomnograph (sleep study). Newer machines are also available in auto-titrating models that allow computer-controlled pressures to be delivered that are automatically adjusted as required during sleep.

Recent advances in masks, humidification, pressure delivery systems, and patient education have greatly improved comfort and adherence to CPAP machines and they are still rated as the most effective medical treatment for severe OSA. Long term compliance with CPAP (>5 years) remains low however, and therefore any person contemplating CPAP should trial or hire a unit for several months before committing to purchase. Places like Gumtree and Ebay are flooded with second hand CPAP units with many still brand new sitting in people’s cupboards.
Surgery
The strategy behind surgical intervention for the treatment of snoring and obstructive sleep apnoea is to open the site of anatomical blockage. The actual blockage site however, may be in more than one place and they are typically found at the nose, soft palate, or base of the tongue. Therefore, some of the better-known procedures such as removal of tonsils, straightening a crooked septum, and trimming of the soft palate (removal of the fleshy bit of the roof of the mouth – UPPP) are routinely carried out.
Other less well known techniques may also be employed such as enlargement of the breathing space behind the tongue, implants into the soft palate, surgical advancement of the mandible or maxilla (lower or upper jaw), or an operation directly on the tongue tendons or the tongue itself. Recent advancements in tongue coblation surgical techniques have helped many people where reduction of the size of the tongue is required to treat OSA.
Surgical techniques are:
– Rhinoplasty, Septoplasty, and Turbinectomy or submucous resection of the turbinates.
– Adenoid and Tonsillectomy.
– Uvulopalatopharyngoplasty (UPPP).
– Somnoplasty, tongue coblation surgery, and Pillar-palato implants.
– Genioglossus advancement.
– Hyoid Suspension.
– Maxillo-mandibular advancement.
– Tracheotomy
Post operative healing of a UPPP.

The majority of these surgical techniques are carried out by an Ear, Nose, and Throat surgeon (ENT), whilst an Oral and Maxillofacial surgeon will perform the jaw advancement surgery. In many cases, surgery alone will not provide complete relief from snoring and OSA symptoms but is often required as a very important part of a comprehensive treatment plan.